The Hidden Map of Mental Health Care Most Americans Never See
When most people picture mental health care, they imagine one image: a person sitting on a couch, talking to a therapist once a week. That picture is not wrong. It is just dramatically incomplete. Behind the familiar weekly therapy hour sits an entire continuum of care, ranging from a fifteen-minute medication check-in to twenty-four-hour residential treatment in a clinical setting. Most Americans never learn this map exists until a crisis pushes them onto it without a guide.
This guide draws that map. You will learn what every level of mental health care actually looks like day to day, who each level is built for, how to know when you should step up to something more intensive or step down to something lighter, and how insurance plans, including UnitedHealthcare therapists and other major networks, actually pay for each step. By the end you will be able to name your current level, describe the next one above and below it, and walk into any conversation with a provider knowing the language they use.
No jargon for the sake of jargon. No false reassurance that one size fits everyone. Just a clear, practical view of the system you are already inside or about to enter.
Why Levels of Care Exist in the First Place
Mental health conditions, like physical conditions, vary enormously in severity. A sprained ankle and a shattered femur are both leg injuries, but one needs an ice pack and the other needs a surgical team. The same logic governs mental health care. A person managing mild seasonal anxiety needs something very different from someone in the middle of a suicidal crisis. Pretending both should sit in the same weekly therapy slot helps neither.
Levels of care are the system’s answer to that variation. Each level represents a different intensity of treatment, measured by how many hours per week you spend receiving care, how much clinical supervision surrounds you, and whether you sleep at home or somewhere else at night. The lower the level, the more your life looks like a normal life with a treatment appointment tucked inside it. The higher the level, the more treatment becomes the structure your life is built around for a defined window of time.
Insurance companies, including the networks behind UnitedHealthcare therapists, organise their coverage around these levels too. They do not pay a flat rate for “mental health treatment.” They pay specific rates for outpatient therapy, for intensive outpatient programs, for partial hospitalisation, for residential care, and for inpatient stays. Knowing which level you are at, and which level your insurance considers medically necessary, is the difference between a treatment plan that gets fully covered and one that leaves you with surprise bills.
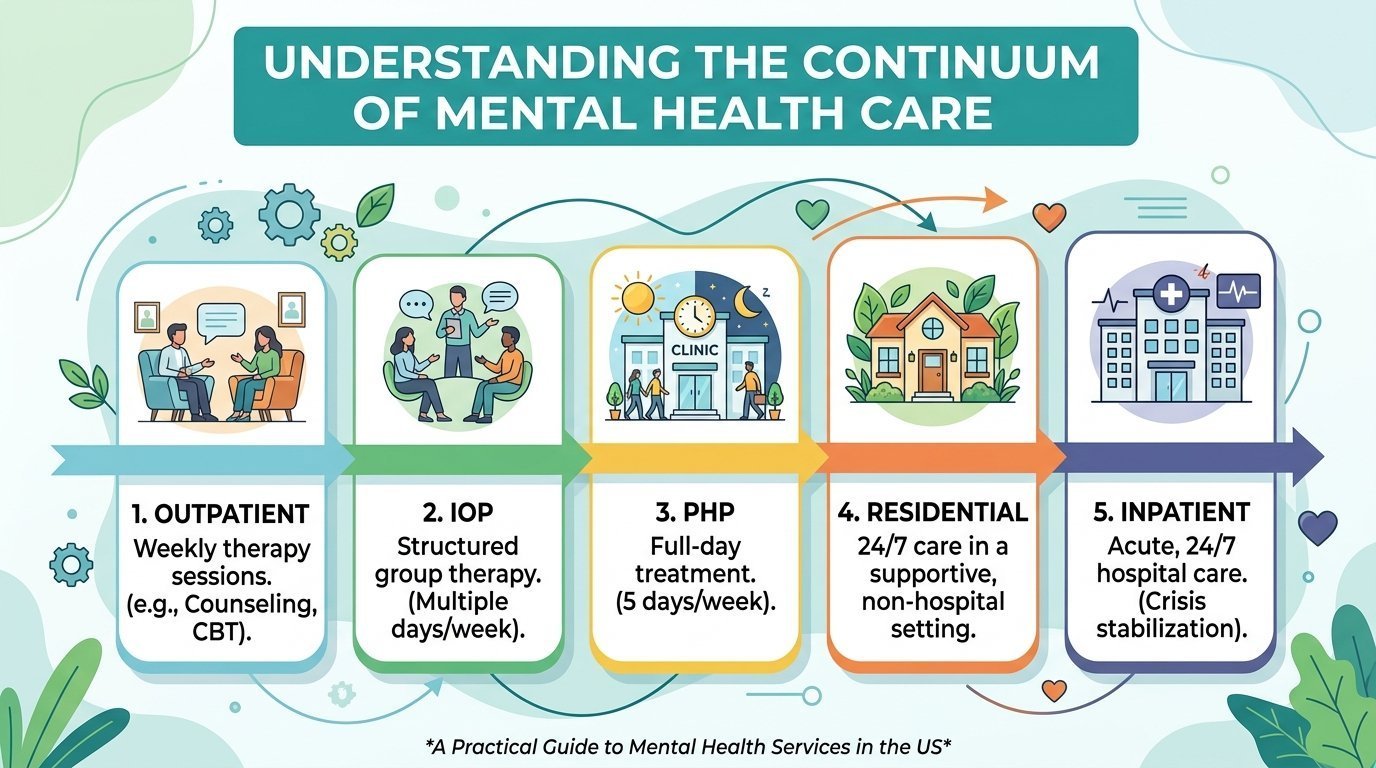
Level One: Standard Outpatient Therapy
This is the picture in most people’s heads. You see a therapist or counsellor once a week, sometimes once every two weeks, for forty-five to sixty minutes per session. You sleep in your own bed every night, work a normal schedule, eat with your family, and fold your therapy appointment into a life that is otherwise running on its usual tracks.
Standard outpatient mental health care is the right fit when your symptoms are stable enough that you can function in daily life, when you have a support system at home, and when the change you are trying to make is gradual rather than urgent. People in this level are managing low to moderate depression, anxiety, relationship difficulties, grief, life transitions, ADHD, mild trauma symptoms, or general stress. They are not in immediate danger. They are not unable to leave the house. They are working on becoming better, not surviving the day.
If you search for mental health providers near me and start scheduling sessions with the first therapist who has openings, you are entering this level by default. Most of America’s three hundred million plus residents who ever receive mental health care in their lifetimes never need anything more intense than this. That is a feature of the system, not a flaw. When weekly outpatient is enough, anything more is unnecessary.
Insurance coverage at this level is the most familiar to most patients. Plans charge a copay, often between twenty and fifty dollars per session, after you meet a deductible. Networks of UnitedHealthcare therapists, Aetna providers, Cigna clinicians, and Blue Cross Blue Shield panels are heavily populated at this tier. Out-of-pocket costs are predictable. The friction is mostly about finding an in-network provider with availability, which can take weeks in some markets.
Level Two: Outpatient Therapy Plus Medication Management
This is still outpatient, but with a second provider added. In addition to your weekly therapy, you also see a psychiatrist or a psychiatric nurse practitioner who manages your medication. The medication visits are shorter, often fifteen to thirty minutes, and less frequent, sometimes monthly and eventually every three months once a regimen is stable.
You move into this level when symptoms are persistent enough that talk therapy alone has not produced enough relief, or when your condition has a strong biological component that responds well to medication, such as moderate to severe depression, generalised anxiety that interferes with sleep and work, panic disorder, bipolar disorder, ADHD, or obsessive-compulsive disorder. Adding medication is not an admission that therapy failed. It is the system using two tools together because two tools do the job better.
Coordination matters here. The therapist and the prescriber should be in communication, even loosely, so that one is not undermining what the other is building. Many integrated practices employ both under one roof. If yours does not, ask both providers to send each other a brief letter once or twice a year. Your treatment will be measurably better for it.
Cost-wise, you are now stacking two services. Therapy copays plus psychiatry copays plus prescription costs. For most plans this is still firmly inside outpatient mental health care insurance benefits, with no preauthorisation needed. Generic versions of common psychiatric medications are inexpensive. Brand-name drugs and newer agents can require a tier exception or a prior-authorisation form, which your prescriber’s office can usually handle in a few days.
Level Three: Intensive Outpatient Programs
This is where the system starts to feel different. An intensive outpatient program, almost universally shortened to IOP, asks you to spend nine to twelve hours per week in structured mental health care, usually delivered in three-hour blocks three days a week. You still sleep at home. You still keep your job in many cases, particularly if your IOP is offered in evening hours, which most are.
What you receive during those nine to twelve hours is a mix of group therapy, individual therapy, psychoeducation, family work, and sometimes medication management folded in. You are part of a small cohort of seven to twelve patients who attend together for the duration of the program, typically six to twelve weeks. The cohort itself becomes part of the treatment. You watch others struggle and recover, and they watch you, and the shared journey is therapeutic in a way that one-on-one work cannot replicate.
People enter IOP for several reasons. Some are stepping up from outpatient because weekly therapy stopped producing improvement and symptoms are worsening. Some are stepping down from a higher level after an inpatient hospitalisation, using IOP as a structured re-entry into normal life. Some present here directly because their condition is too severe for once-a-week care from the start, including substance-use disorders, eating disorders, severe depression, severe anxiety with significant functional impairment, and post-traumatic stress disorder.
Insurance coverage at this level requires a clinical justification. The IOP intake team writes a treatment plan documenting why nine-plus weekly hours of mental health care is medically necessary, and the insurer reviews it. Networks like UnitedHealthcare therapists and Optum behavioural health typically approve IOP in increments, authorising two to four weeks at a time and requiring continued-stay reviews afterwards. Out-of-pocket costs vary widely. Some plans cover IOP under your behavioural health benefit at the same copay as standard outpatient. Others apply a higher cost share. Always confirm before starting.
Level Four: Partial Hospitalisation Programs
A partial hospitalisation program, almost always called PHP, is what people mean when they say “day treatment.” You attend a clinical setting for six hours a day, five days a week, for two to four weeks on average. You eat lunch there. You spend most of your waking weekday hours there. You sleep at home each night, which is the only reason it is called partial.
The intensity of treatment at this level is approaching what an inpatient unit provides, minus the overnight stay. You receive multiple group therapy sessions per day, daily individual check-ins, medication management built into the schedule, and structured activities including dialectical behaviour therapy skills training, cognitive behavioural therapy modules, art or expressive therapies, and family sessions one or two times during the program.
PHP is the right level when your symptoms are too severe for IOP but not severe enough that you need the safety of an inpatient unit. People presenting with suicidal thoughts that they can manage with support, severe depressive episodes, post-discharge stabilisation after an inpatient stay, severe eating disorders that need daily monitoring of meals, or moderate-to-severe substance-use disorders requiring intensive structure all benefit from PHP. So do people who started in IOP and are not making sufficient progress.
Most people who complete PHP step down into IOP for several weeks before returning to standard outpatient mental health care. The graduated reduction matters. Going directly from six clinical hours a day to one therapy session a week is a cliff that many patients cannot navigate without slipping. Insurance plans understand this and increasingly authorise PHP and IOP as a connected continuum rather than treating them as isolated decisions.
Level Five: Residential Treatment
At the residential level, you live at the treatment centre. You sleep there. You eat there. Your daily schedule is built by clinicians, not by you. Stays last anywhere from twenty-eight days to several months, depending on the diagnosis and the program. You bring a small bag of belongings, you surrender your phone for portions of the day, and you submit yourself to a complete environmental change designed to interrupt patterns that outpatient and partial care could not interrupt.
Residential treatment is most common for substance-use disorders, severe and treatment-resistant eating disorders, severe trauma and PTSD, complex co-occurring disorders where mental illness and addiction reinforce one another, and adolescents whose home environment is itself part of what is keeping them unwell. It is not, despite the cultural impression created by celebrity coverage of “rehab,” a luxury experience for the lightly distressed. It is a serious clinical intervention reserved for serious clinical situations.
The cost of residential mental health care is the highest in the outpatient continuum, often twenty to fifty thousand dollars for a typical thirty-day stay before insurance. Coverage is highly variable. Some plans cover residential at the same level as inpatient hospitalisation. Others cap covered residential days per year. Out-of-network residential treatment can leave families with five-figure surprise bills even when the program is reputable. Always, without exception, get insurance preauthorisation in writing before admission. If a residential program tells you they will “verify benefits” but cannot produce a written authorisation, treat that as a financial red flag.
Level Six: Inpatient Hospitalisation
Inpatient psychiatric hospitalisation is the highest level of acute mental health care. You are admitted to a locked unit, usually inside a general hospital or a free-standing psychiatric facility, where psychiatric nurses and physicians provide twenty-four-hour clinical coverage. The average length of stay in the United States is short, between three and seven days, because the goal of inpatient treatment is stabilisation, not long-term recovery.
You arrive at this level for one of three reasons. You are an immediate danger to yourself, usually meaning active suicidal intent or behaviour. You are an immediate danger to others, which is rarer than media coverage suggests but does happen during certain manic, psychotic, or substance-induced states. Or you are unable to care for yourself due to severe psychiatric symptoms, including catatonia, severe psychosis, or extreme manic episodes. Inpatient is the system’s safety net. It is not a longer or more thorough version of outpatient. It exists to keep you alive and functioning long enough that step-down levels can do the actual recovery work.
Admission can be voluntary, where you sign yourself in, or involuntary, where a clinician, family member, or law-enforcement officer initiates a hold based on state-specific civil commitment laws. Voluntary admissions are always preferable when possible, because they preserve your sense of agency and your insurance pays them at the same rate. Involuntary holds in most states last seventy-two hours and require a formal hearing if extended. If you or a loved one are facing an involuntary hold, learn your state’s specific process and your right to legal representation. The 988 Suicide and Crisis Lifeline can connect you with mobile crisis teams that often prevent the need for inpatient admission entirely.
Insurance is required by federal mental health parity law to cover inpatient psychiatric hospitalisation at the same level it covers inpatient medical hospitalisation. In practice, that means your hospital deductible and co-insurance apply just as they would for an appendectomy. Networks like UnitedHealthcare therapists, Aetna, and Anthem cover the full medically necessary stay, although they review for continued-stay justification daily and will press for discharge to a step-down level as soon as criteria are met. Most patients leave inpatient and step down to PHP, then IOP, then standard outpatient mental health care over a span of several weeks.
How to Know You Need to Step Up
Patients are surprisingly bad at recognising when they need a higher level of care. Symptoms creep, weeks blur into months, and the threshold where outpatient stops being enough is hard to feel from inside the experience. A few clear signals that it is time to ask your therapist or psychiatrist about stepping up:
You are missing work, school, or major life responsibilities multiple times a week because of mental health symptoms. You have been in standard outpatient for three or more months without measurable improvement, despite engaged participation. You are using alcohol or drugs more frequently or in larger quantities to manage emotional pain. You are having thoughts of suicide or self-harm with any frequency, even if you are not making active plans. You cannot eat regularly, cannot sleep more than a few hours, or cannot leave the house. Family members or close friends are independently expressing concern about your safety. Any of these on their own may not require a higher level. Two or three together usually do.
If you recognise yourself in this list, the right move is not to wait until your next scheduled session. It is to call your provider and say the words: I think I might need a higher level of care. Most mental health providers near me will respond same-day to that phrase. Many practices have direct relationships with IOP and PHP programs and can make a warm referral within a few business days. Insurance preauthorisation usually takes seventy-two hours or less for IOP and PHP admissions. The system can move quickly when you give it the right signal.
How to Know You Are Ready to Step Down
Stepping down is its own skill. Patients who have benefited from intensive mental health care sometimes cling to it past the point where it is helping, treating the program as a structure that holds them up. The clinical team will signal readiness by reducing your individual session frequency, encouraging you to take on more outside-of-treatment responsibilities, and discussing discharge timelines openly with you. When that conversation begins, lean into it.
Concrete signs that you are ready to step down: you have not had a safety crisis in several weeks, your sleep and appetite have stabilised, you can identify your triggers and name the coping skills you would use, you have a written safety plan you actually believe in, and you have built a support system outside the program walls. The goal of every level above standard outpatient is to make itself unnecessary. A successful stay at PHP ends not with a permanent attachment to the program but with a confident return to life.
Insurance, Costs, and the Conversations Most Patients Skip
The single most expensive mistake patients make as they move between levels of mental health care is failing to have an explicit, documented conversation with their insurance plan before each transition. Treatment teams will often handle preauthorisation for you, but the contract is between you and the insurer. You are the one who pays the bill if something falls through.
Before any step up to IOP, PHP, residential, or inpatient, call the member-services number on the back of your insurance card and ask three specific questions. Is the program in network. What is the preauthorisation status of my admission. What is my expected out-of-pocket cost for the full course of treatment. Write down the representative’s name, the date and time, and a reference number for the call. If your plan is one of the major networks like UnitedHealthcare therapists, Optum behavioural health, Aetna, Cigna, or a Blue Cross Blue Shield variant, this call is routine for them and should take fifteen to twenty minutes.
If a program tells you that calling your insurance is not necessary because they will “handle everything,” do it anyway. Programs are not legally responsible for your insurance contract. They are responsible for delivering care. Closing that loop yourself, in writing, is a five-figure decision for higher levels of care and a four-figure decision for IOP. It takes one phone call.
Special Situations the Standard Continuum Does Not Cover
Several patient populations need mental health care that does not fit neatly into the six levels above. Veterans receiving care through the VA navigate a parallel system with its own intensity tiers and its own community-care referral process. Children and adolescents have age-adjusted versions of every level, including school-based partial programs and adolescent-specific residential treatment. Pregnant and postpartum patients increasingly have access to perinatal-specialised IOPs and PHPs that integrate obstetric care with mental health treatment. Patients with serious mental illness like schizophrenia or schizoaffective disorder often participate in assertive community treatment teams that bring intensive outpatient services to their home.
If your situation falls into one of these categories, ask explicitly when you search for mental health providers near me. The standard intake clerk at a general practice may not know the specialised programs available in your region. State behavioural health authorities, county-level community mental health centres, and disease-specific advocacy organisations such as NAMI, the National Alliance on Mental Illness, can shorten the search dramatically.
A Final Word: The Map Is Not the Territory
Every diagram of levels of care in mental health care makes the system look cleaner than it is. In real life, levels overlap, programs blend, and the same patient may need different levels for different conditions over the course of a year. A person with co-occurring depression and substance use may be in standard outpatient for therapy while also attending an IOP for substance use, with a separate medication-management appointment with a third clinician. The neat ladder turns into a constellation.
That complexity is not a sign you are doing it wrong. It is a sign that the system is finally tailored to a real human life rather than a textbook diagnosis. The map exists to give you language and orientation, not to dictate a single linear path. Walk into your next provider conversation knowing the words. Ask which level you are at, where you might step next, and why. Treatment that you understand is treatment that you can finish.
This article is for educational purposes and does not replace personalised guidance from a licensed mental health clinician. If you or someone you know is in crisis, call or text 988, the Suicide and Crisis Lifeline, available twenty-four hours a day in the United States. For coverage questions, contact your insurance plan directly using the member-services number on the back of your card.